Blood Gas Analysis
Arterial blood gas analysis the "gold standard" to analyze ventilation and perfusion.
Acid - Base status
PH of arterial blood is determined primarily by :
1.PaCO2 indicates adequacy of ventilation.
2.Lactic acid , produced by anaerobic metabolism
3.Buffering capacity, determined by the amount of bicarbonate in the blood.
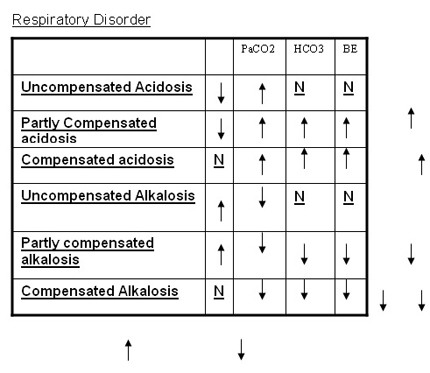
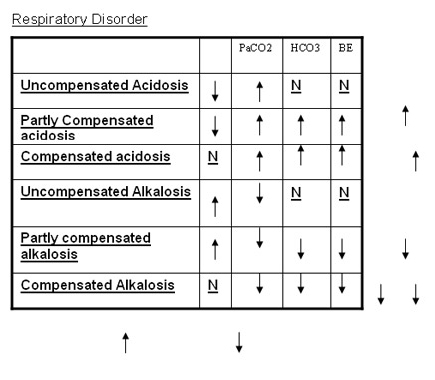
Respiratory disorders
Respiratory acidosis occurs when an increase in PaCO2 causes a decrease in pH.
Respiratory alkalosis occurs when a decreases in PaCO2 causes an increase in pH.
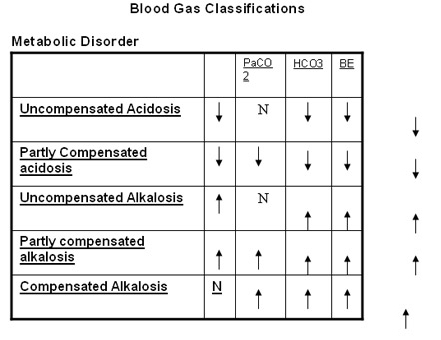
Metabolic disorders
Metabolic acidosis occurs when there is either an excess of lactic acid or a deficiency in the buffering capacity of the blood, causing a decease in pH. It is reflected in an increased base deficit ,also termed a decreased base excess. ( Normal range of base deficit < -8).
Compensation in acid base disturbances
.If PaCO2 remains persistently elevated(respiratory acidosis), the pH will gradually tend to return towards normal as a result of a gradual increase in bicarbonate in the blood, termed compensatory metabolic alkalosis. .Conversely, a patient with a persistently low PaCO2(respiratory alkalosis) will gradually develop compensatory metabolic acidosis .In patients with an intact respiratory drive, persistent metabolic acidosis will result in hyperventilation termed compensatory respiratory alkalosis.
Choose the appropriate compensation formula
? indicates -unit change
If the pH and pCO2 do not follow the expected correction a mixed disorder is to be expected
Basic Questions in analysis of ABG
Interpretation:
pH: Is it normal, acidotic, or alkalotic?
PCO2: Is it normal, (respiratory acidosis), or (respiratory alkalosis)?
HCO3: Is it normal, (metabolic acidosis), or (metabolic alkalosis)?
Simple disorder or mixed? Compensated or not?
PO2: Normal, hypoxia, or hyperoxia
Blood Gas Classifications
BE -Base excess; , elevated Values; depressed Values; N, normal
Error in Blood Gas Measurements 1.An air bubble in a blood gas sample will cause blood to equilibrate with room air.
.PaCO2 will be artificially lowered
.PaO2 will move closer to the partial pressure of O2 in room air (approx 140mmhg)
2. Dilution of a blood gas sample with IV fluid will cause both CO2 & O2 to diffuse from blood in to the diluting fluid.
.PaO2 & PaCO2 will be artificially lowered
.Because of buffering capability of blood , pH will not change as much as will PaCO2.The combination of relatively normal pH and decreased PaCO2 will appear to be respiratory alkalosis with metabolic acidosis .
3. If blood gas sample is kept for along period at room temperature, the blood cells will continue to metabolize oxygen and produce CO2.
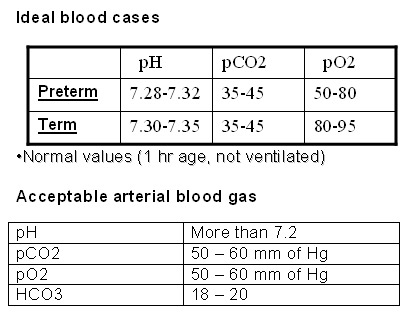
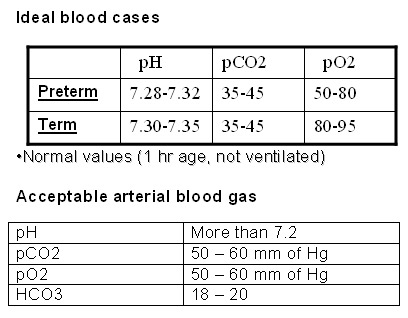
Ideal blood cases
Normal values (1 hr age, not ventilated)
Acceptable arterial blood gas
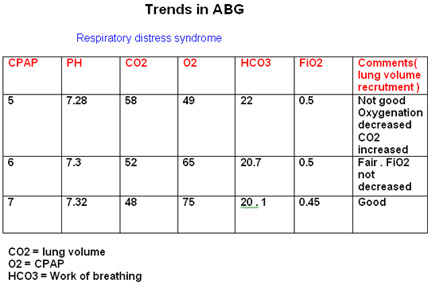
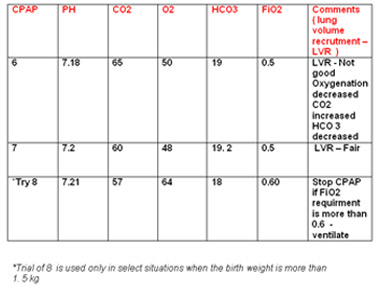
Trends in ABG
Respiratory distress syndrome
CO2 = lung volume
O2 = CPAP
HCO3 = Work of breathing
*Trial of 8 is used only in select situations when the birth weight is more than 1. 5 kg
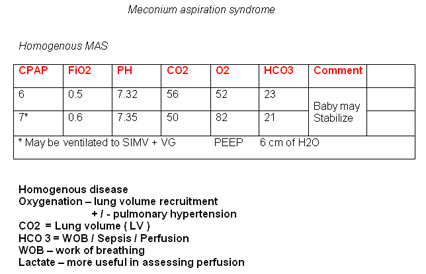
Meconium aspiration syndrome
Homogenous MAS
Homogenous disease
Oxygenation - lung volume recruitment + / - pulmonary hypertension
CO2 = Lung volume ( LV )
HCO 3 = WOB / Sepsis / Perfusion
WOB - work of breathing
Lactate - more useful in assessing perfusion
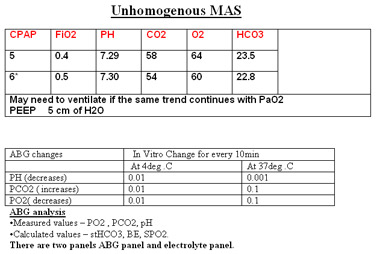
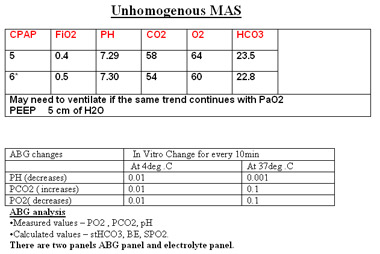
Unhomogenous MAS
ABG analysis .Measured values - PO2 , PCO2, pH
.Calculated values - stHCO3, BE, SPO2.
There are two panels ABG panel and electrolyte panel.
.Electrolyte panel shows measured HCO3
. while ABG panel shows st.HCO3 which is calculated HCO3 keeping Pco2 =40mmHg and temp at 37deg as constant.
.Under ideal condition-SBC = HCO3 = +/- 2mEq
.SBC low- metabolic acidosis
.SBC high- metabolic alkalosis
.Difference b/n actual HCO3 and SBC indicates- respiratory cause
.HCO3> SBC respiratory acidosis
.HCO3< SBC respiratory alkalosis
Principle of ABG analysis
.pH and HCO3 moves in same direction
.pH and PCO2 moves in opposite directions
.HCO3 and PCO2 moves in same direction in simple disorders and in opposite directions in mixed disorders
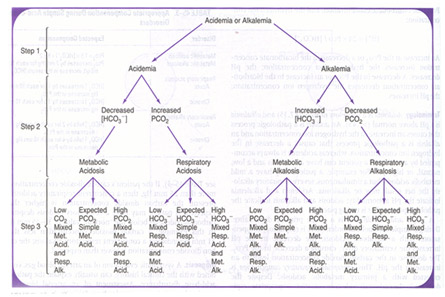
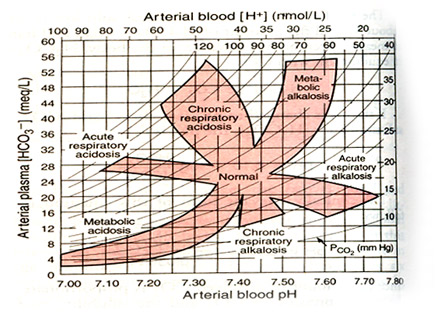
Interpretation of ABG.
FIVE STEP METHOD OF DEOSTAT
1) LOOK FOR pH
2) WHO IS THE CULPRIT ?
3) IF RESPIRATORY ACUTE / CHRONIC- COMPENSION ?
4) IF METABOLIC / COMPENSATION / ANION GAP
5) CLINICAL CORRELATION
The Henderson-Hasselbalch Equation:
[H+] = 24 x [pCO2/ HCO3]
pH = 6.1 + log [HCO3] / [0.0301 x pCO2]
pH = 6.90 7.00 7.10 7.20 7.30 7.40 7.50 7.60
[H+]= 125 100 80 64 51 40 32 25
Crudely PCO2 = 80 - Decimal number in pH
Eg - pH = 7.30, PCO2 = 80 - 30 = 50
Normal Lung , PO2 = FiO2 x 4
Rules for Respiratory Acid-Base Disorders
1. The [HCO3] will increase by 1 mmol/l for every 10 mmHg elevation in pCO2 above 40 mmHg. Expected [HCO3] = 24 + { (Actual pCO2 - 40) / 10 }
Comment:The increase in CO2 shifts the equilibrium between CO2 and HCO3 to result in an acute increase in HCO3. This is a simple physicochemical event and occurs almost immediately.
Example: A patient with an acute respiratory acidosis (pCO2 60mmHg) has an actual [HCO3] of 31mmol/l. The expected [HCO3] for this acute elevation of pCO2 is 24 + 2 = 26mmol/l. The actual measured value is higher than this indicating that a metabolic alkalosis must also be present.
2. The [HCO3] will increase by 4 mmol/l for every 10 mmHg elevation in pCO2 above 40mmHg. Expected [HCO3] = 24 + 4 { (Actual pCO2 - 40) / 10}
Comment: With chronic acidosis, the kidneys respond by retaining HCO3, that is, renal compensation occurs. This takes a few days to reach its maximal value.
Example: A patient with a chronic respiratory acidosis (pCO2 60mmHg) has an actual [HCO3] of 31mmol/l. The expected [HCO3] for this chronic elevation of pCO2 is 24 + 8 = 32mmol/l. The actual measured value is extremely close to this so renal compensation is maximal and there is no evidence indicating a second acid-base disorder.
3.The [HCO3] will decrease by 2 mmol/l for every 10 mmHg decrease in pCO2 below 40 mmHg. Expected [HCO3] = 24 - 2 { ( 40 - Actual pCO2) / 10 }
Comment: In practice, this acute physicochemical change rarely results in a [HCO3] of less than about 18 mmol/s. (After all there is a limit to how low pCO2 can fall as negative values are not possible!) So a [HCO3] of less than 18 mmol/l indicates a coexisting metabolic acidosis
4.The [HCO3] will decrease by 5 mmol/l for every 10 mmHg decrease in pCO2 below 40 mmHg. Expected [HCO3] = 24 - 5 { ( 40 - Actual pCO2 ) / 10 } ( range: +/- 2)
Comments:
. It takes 2 to 3 days to reach maximal renal compensation
. The limit of compensation is a [HCO3] of about 12 to 15 mmol/l
5.The expected pCO2 (in mmHg) is calculated from the following formula: Expected pCO2 = 1.5 x [HCO3] + 8 (range: +/- 2) Comments:
. Maximal compensation may take 12-24 hours to reach
. The limit of compensation is a pCO2 of about 10 mmHg
. Hypoxia can increase the amount of peripheral chemoreceptor stimulation
Example: A patient with a metabolic acidosis ([HCO3] 14mmol/l) has an actual pCO2 of 30mmHg. The expected pCO2 is (1.5 x 14 + 8) which is 29mmHg. This basically matches the actual value of 30 so compensation is maximal and there is no evidence of a respiratory acid-base disorder (provided that sufficient time has passed for the compensation to have reached this maximal value). If the actual pCO2 was 45mmHg and the expected was 29mmHg, then this difference (45-29) would indicate the presence of a respiratory acidosis and indicate its magnitude.
6.The expected pCO2(in mmHg) is calculated from the following formula: Expected pCO2 = 0.7 [HCO3] + 20 (range: +/- 5)
Comment: The variation in pCO2 predicted by this equation is relatively large
Maximum compensation
In Metabolic acidosis-PaCO2 = Up to 10
In Metabolic alkalosis-PaCO2 = Maximum 60
In Respiratory acidosis-BICARB = Maximum 40
In Respiratory alkalosis-BICARB = Up to 10-12
Consider more than one disorder if
- pH normal ,and PCO2 and HCO3 out of range
- PCO2 and HCO3 moving in opposite directions
- Degree of compensation inappropriate for primary disorder.
- Review with proper clinical history
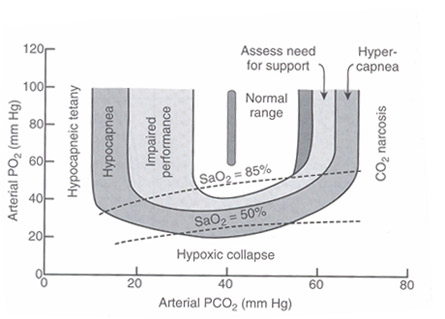
Arterial blood gases application
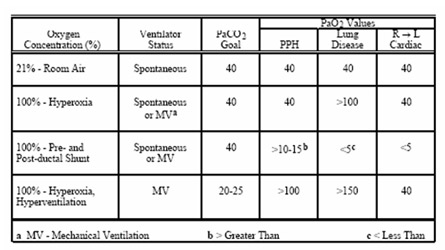
1)Hyperoxia test- Cyanotic neonate
Normal PaO2 =104.2 - (0.27 x age)
. At FiO2 100% if PaO2 above 100mmHG -excludes most cyanotic congenital heart defects
. Always do simultaneous Right radial and post ductal ( posterior tibial) PaO2
. Right radial exceeds post-ductal PaO2 by 10-20 mmHg in persistent pulmonary hypertension
. Pulse oximetry: Preductal (right finger) oxygen saturation (SaO2) exceeds postductal (toe) SaO2 by =5% suspect PPHN
. PaO2 improvement with Hyperventilation targeting PCO2 < 30mm Hg (Respiratory alkalosis) may be helpful differentiating PPHN from CCHD
. Severity of Hypoxia on ventilated baby can be assessed by Oxygenation index .
Oxygenation Index = (MAP x FIO2 x 100) = 40-45 normally postductal PaO2
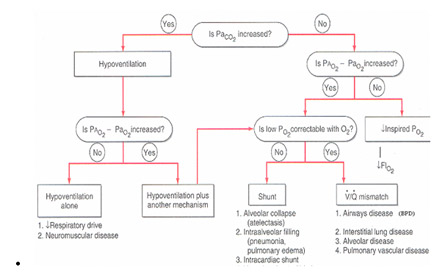
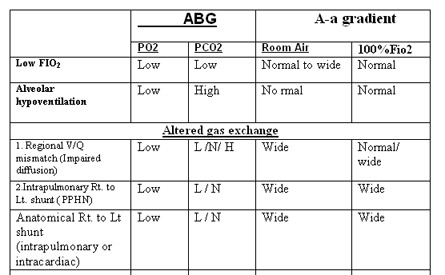
2)Alveolar-arterial O2 tension difference/gradient
P(A-a) O2 = (713 x FiO2 - 1.25 x pCO2) - PaO2
. For Room air FiO2 = 0.21, remember( 713 x 0.21 - 45 ) - 85
. (Normal A-a gradient 10-15 mmHg)
. For 100% O2 FiO2 = 1.0 (Normal A-a gradient 100-150 mmHg);
For each 5% AV shunt, A-a gradient decreases about 100 mmHg below 600 mmHg at FiO2= 1.0
. (A-a)DO2 determination helps to determine if hypoxia is due to poor ventilation(due to inc in PaCO2 ) or due to deficiency of oxygenation.
. O2 has higher alveolar concentration than arterial concentration as against CO2 which freely diffuses across lung.
. Increase in CO2 (as in hypoventillation) will displace the O2 in alveolu
Application of ABG in neonatology
Case 1 -
Cord pH to document significant perinatal asphyxia Definition used as an essential criterion is pH less than 7.00 and base deficit (bicarbonate [HCO3]) greater than 12 mmol/L
Intrapartum asphyxia, defined as acute interruption of oxygen supply,commonly occurs when the placenta, for one reason or another, is hypoperfused.In such a circumstance, retention of carbon dioxide (CO2) occurs. Because the fetus normally clears CO2 by way of the placental circulation, the finding of increased partial pressure of CO2 (PCO2) in the cord blood analysis is a marker of respiratory acidosis. In contrast to the adult, if the asphyxia is not corrected, metabolic acidosis eventually develops and creates a state of mixed respiratoryand metabolic acidosis. Over time, the respiratory component dissipates and,finally, almost pure metabolic acidosis is found.
In all these phases, acidemia is present (ie, a low pH is found in the bloodsample). The cutoff value for damaging acidosis is set at pH less than 7.00 because it is unlikely that acute acidosis with pH values greater than 7.00 could be directly associated with CP. Moreover, because respiratory acidosis is of little consequence in terms of outcome, the metabolic component of damaging acidemia is of importance. Hence, the definition used as an essential criterion is pH less than 7.00 and base deficit (bicarbonate [HCO3]) greater than 12 mmol/L The final pH of blood is determined by the proportion between the PCO2 (respiratory) component and the HCO3 (metabolic) component. This construct suggests that when metabolic acidemia is found, the timing of the hypoxic insult cannot be estimated. In contrast, when a respiratory component is found, the onset of hypoxic insult can be established because this component cannot last more than 20 to 30 minutes (usually less).
Furthermore, one can establish what the pH was before the acute insult by reducing the respiratory component. This calculation can be performed by the method described by Eisenberg and colleagues
In the first step, one subtracts the value of the normal neonatal PCO2 (50 mm Hg) from the PCO2 value found in the blood gas analysis to establish the excess in CO2. Next, given that every 10 mm Hg of the PCO2 reduces the pH by 0.08, the excess PCO2 is divided by 10 and multiplied by 0.08. Finally, the resultant respiratory acidosis component is added to the pH to establish the mixed acidosis level.
For example, an acute hypoxic event occurred during labor and the attending physicians rushed the patient for a prompt cesarean. The baby was delivered within 14 minutes. The claim was that the attending staff overlooked signs of fetal distress before the hypoxic event that prompted the cesarean. Cord blood gases showed a pH of 6.90 and a PCO2 of 100 mm Hg. Using the previously mentioned calculation, the excess of PCO2 is 100 _ 50 ¼ 50 mm Hg. The respiratory acidosis level is calculated as 50 O 10 ¼ 5 _ 0.08 ¼ 0.4. From this cord gas level, one can deduce that the pH before respiratory acidosis started was 6.90 þ 0.4 ¼ 7.30, a perfectly normal value.Thus, the allegation that a nonreassuring fetal heart rate tracing was present before the acute hypoxic event is very unlikely.
Another example describes a patient admitted to the hospital with a nonreassuring admission fetal heart rate tracing. After some initial observation, the patient was rushed for a prompt cesarean. The claim was that damage occurred after admission. Cord blood gases showed a pH of 6.90 and a PCO2 of 60 mm Hg. Using the same calculation, the excess of PCO2 is 60 _ 50 ¼ 10 mm Hg and the respiratory acidosis level is 10O10 ¼ 1 _ 0.08 ¼ 0.08, for a pH value of 6.90 þ 0.08 ¼ 6.98, a level considered damaging acidemia. These cord blood gases, uncorrected by a respiratory component, cannot support a recent asphyxia event; in fact, they cannot tell us when the damaging acidemia occurred.
Case 2
A term AGA male baby was delivered by emergency LSCS in view of thick MSAF . Baby was vigorous at birth with good heart rate and tone. Oropharyngeal suction was given and stomach wash given . Cord pH was 7.2 , base deficit of 12 was noted . Baby was shifted to NICU for observation in view of thick MSAF and mild tachypnea .
Baby was nursed under warmer ,O2 was given through hood for mild tachypnea .and Iv fluids was started. Over next 4-6hrs respiratory distress increased and baby had frequent desaturation with Spo2 dipping below 85% on 6lt O2 hood. And baby turning completely cyanotic with mild displacement of O2 hood and stimulation during oropharyngeal suction.There was more than 5% difference in upper limb and lower SPo2..Chest x-ray showed b/l perihilar haziness with loss of lung volume ( 6 ICS ).Baby was intubated inview of impending repiratory failure.
Even on 100% Fio2 SPo2 did not improve more than 92% in Rt.upperlimb and was 85% in lower limb. Baby was completely sedated Hyperoxia test performed and simulataneous ABG form preductal ( rt.radial) and post ductal ( lower limb) were taken which showed PO2 of 60 and 40mmHg respectively and difference 20mmHg .So PPHN was suspected .
Hyperventilation test by increasing rates and PIP, to target PCO2 of 30-35 mm Hg and respiratory alkalosis was preformed which showed improvement in Po2 to 150mmHg .
Line of management -
Echo - to rule out CCHD , to determine severity of PPHN and to document pulmonary gradient.
To target Systemic pressure above pulmonary arterial pressure( so as to prevent Rt- left shunt across PDA and PFO ) with Fluid bolus and Inotropes support.
Maintain Euthermia , euvolumia and euglycemia.
Minimum stimulation and adequate sedation
Avoid hypotension and hypoxic events- Ionotropes, 100% Fio2
Gentle ventilation with optimum PEEP and PIP
Case 3
CDH
Permissive hypercapnea
Permissive hypercapnea was a novel strategy used in mechanically ventilated babies to reduce the incidence of chronic lung disease
. Current understanding of this strategy dictates that any pCO2 more than 55 and a pH less than 7.2 is to be treated with great caution with regards to neurodevelopmental outcome . We could accept CO2 in the 70s in the early part of treatment of RDS if it shows a diminishing trend . The author has been applying this principle since 1997 and concludes with the simple statement that we should not chase ideal blood gases if the baby is hemodyanamically stable . This concept of permissive hypercapnea should ideally not be used in the acute phase of lung disease ( FiO2 more than o.6 )
PH
Important Trends in ABG
The author feels that improvement in PH , usually parallels improvement in respiratory status and work of breathing . Deterioration in pH , even if doesn't meet protocol criteria ( pH >7.2 and CO2 60mm Hg) should be taken as an indication to intervene by mechanical ventilation especially if the respiratory distress scoring is deteriorating or the baby appears pale
with increased CFT
Assessment of gas exchange
ABG is the most common tool to assess gas exchange . however , the target oxygen tensions that should be achieved is still controversial .with high ventilary rates and high pressures , one may achieve any desired gas values for a while . the aim should be to attain adequate gas exchange without causing barotraumas . neonates will be well oxygenated if PaO2 is maintained between 50 and 70 mm of hg ( 6.7 to 9.3 Kpa ) . hence mechanical ventilation is an individualized maneuvour . It has been showed that a permissive hypoxia and permissive hypercapnea reduces the incidence of bronchopulmonary dysplasia .However , in term infants , the chances of pulmonary hypertension is more possible and hence a PaO2 of 60 to 80 mm of Hg is preferable ( 8 to 10 Kpa ) The PaCo2 in a healthy term infant in the first 24 hours of life is about 33.4 + / - 3.1 mm of Hg . However the need to hyperventilate to achieve this value is not advocated .
Back