Ventilator Graphics
Graphics are waveforms that reflect the patient-ventilator system and their interaction
Role of ventilator wave forms
. Identify pathophysiologic processes
. Recognize patients response to therapy and monitors patients disease status
. Calculate respiratory mechanics
. Optimise ventilator settings and treatment
. Determine effectiveness of ventilator settings
. Detect adverse effects of mechanical ventilation
. Minimize risk of ventilator induced complications - Allows user to interpret,
evaluate, and troubleshoot ventilator and patients' response to ventilator
Ventilator Graphic classification
1) Scalar graphic - Any single variable (eg-Flow, pressure, volume) plotted
against time.
a) Flow vs time scalar
b) Pressure vs time scalar
c) Volume vs time scalar
2) Loops - The two dimensional graphic display of two scalars
a) Pressure-Volume loop
b) Flow-Volume loop
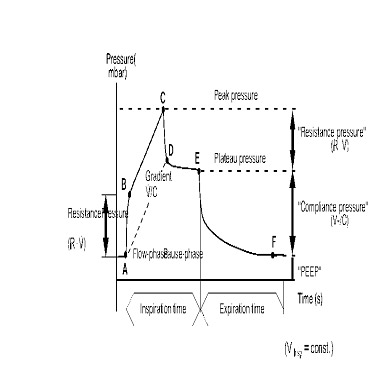
Pressure waveforms
. Rectangular waveform
. Exponential rise wave form
. Sine wave form
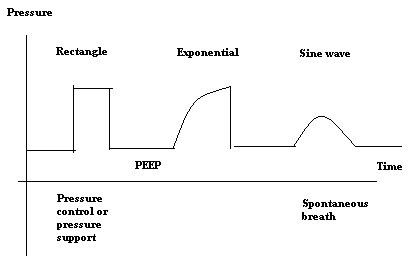
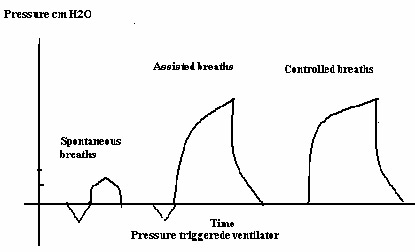
.Machine-triggered breaths have no negative deflection at the start
.Patient triggered breaths may have a negative deflection at the start if the breath is being pressure triggered.the greater the patient effort to trigger the breath, the greater the negative deflection seen.no deflection see with flow triggering
.In volume modes, the shape will be exponential rise for mandatory breaths and sinusoidal for spontaneous breaths.if PS is added to spontaneous breaths, then the waveform will be square on the spontaneous breaths
.In pressure modes, the shape will be rectangular for mandatory breaths and sinusoidal for spontaneous breaths.if PS added to the spontaneous breaths, they will be rectangular also
.If PEEP is added, the baseline during expiration will be above zero
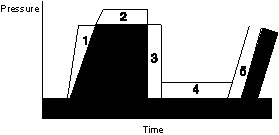
.The area under the entire curve equals the Paw (mean airway pressure)
To Increase Mean Airway Pressure
1. Increase flow
2. Increase peak pressure
3. Lengthen inspiratory time
4. Increase PEEP
5. Increase Rate
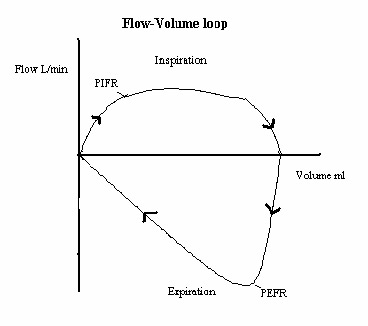
.Flow is plotted on the y axis and volume on the x axis
.Inspiration is above the horizontal line and expiration is below (some vents reverse this and I is below while E is above)
.The shape of the inspiratory flow curve will match what's set on the ventilator
.The shape of the expiratory flow curve represents passive exhalation.it's long and more drawn out in patients with less recoil
.Can be used to determine the PIFR, PEFR, and Vt
.Looks circular with spontaneous breaths
.Looks squared but set at an angle with PC/PS breaths
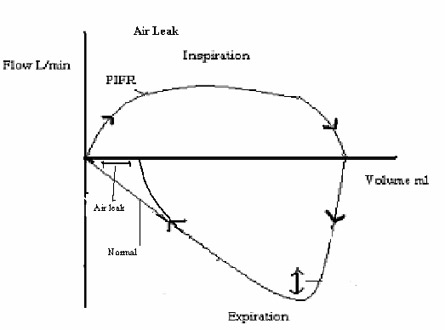
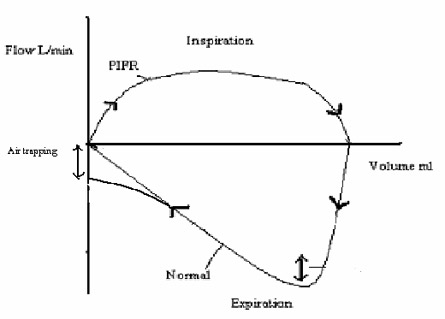
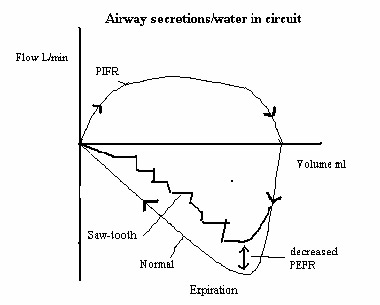
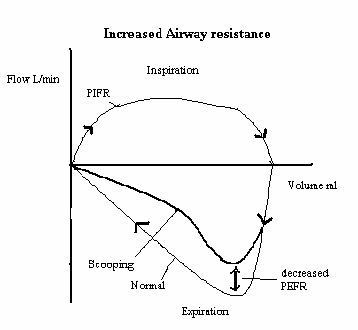
Abnormal FV Loops
.The expiratory curve "scoops" with high expiratory resistance
.If the patient is air trapping or has a leak, the loop will not meet at the left side where I starts/E ends
.If water/secretions are building up in the airway or circuit, the loop becomes very jagged
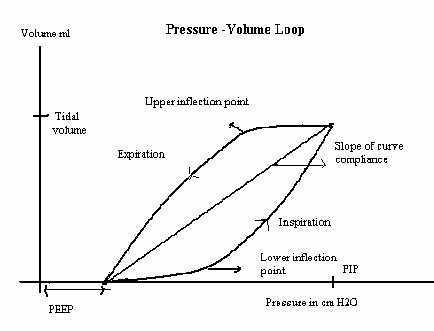
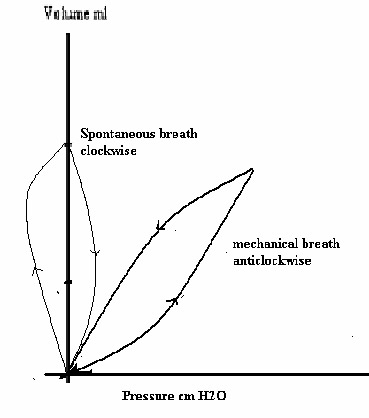
.Volume is plotted on the y axis and pressure on the x axis (can also be plotted the other way around)
.Inspiratory curve is upward and expiratory curve is downward
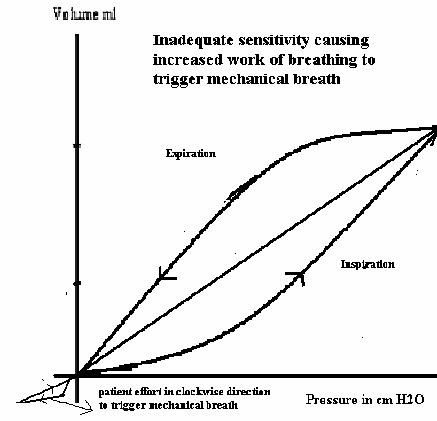
.Spontaneous breaths go clockwise and positive pressure breaths go counterclockwise
.The bottom of the loop will be at the set PEEP level or be at 0 if there's no PEEP set
.I starts and E ends at the bottom of the loop.I ends and E starts at the top of the loop
.The loop is almost square in PC/PS because of pressure limiting during I
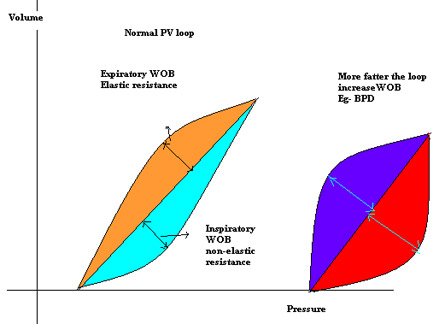 Abnormal PV Loops
Abnormal PV Loops
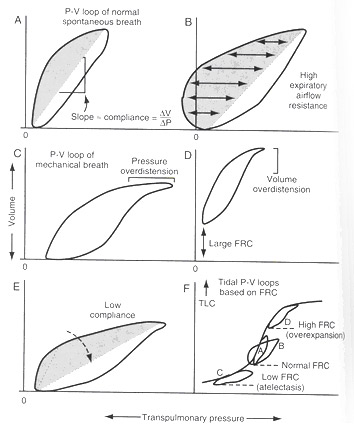
.If an imaginary line is drawn down the middle of the loop, the area to the right represents inspiratory resistance/WOB and the area to the left represents expiratory resistance/WOB (just the opposite for spont breaths- I is to the left and E is to the right)
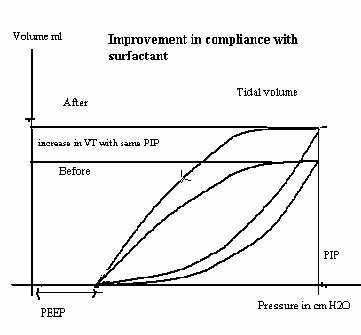
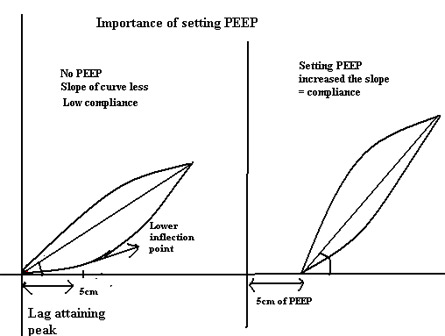
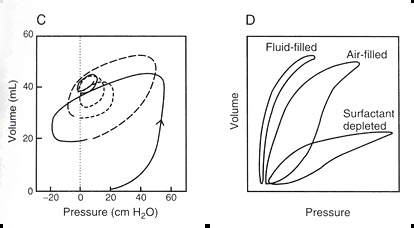
.The more vertical the loop lays, the higher the lung compliance, the more horizontal it lays, the lower the lung compliance. Thus slope of the line equals compliance.
.The fatter the loop, the higher the airway resistance.you can tell if it's I or E resistance by looking at whether the right or left side bulges out more
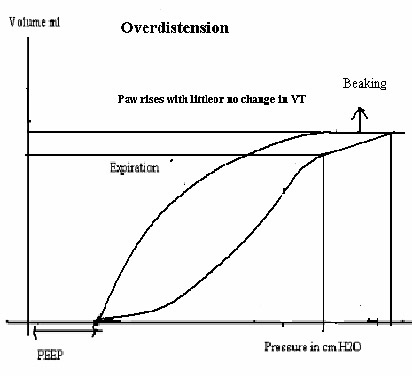
.A bird beak at the top of the loop represents over-distension
.A pig tail at the bottom indicates patient triggering.the bigger the pig tail, the higher the patient WOB to trigger the breath
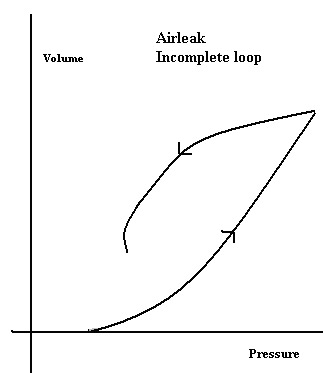
.The loop won't meet at the bottom with airtrapping or leaks
Example -
Inspiratory WOB-Increased secretion, Kinked or partially blocked tube.
Expiratory WOB - Bronchospasm , BPD lung
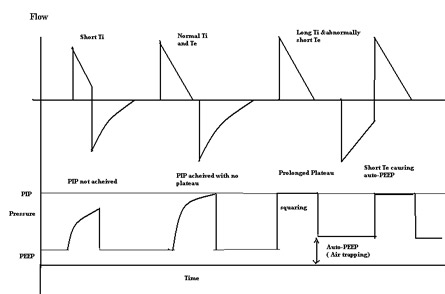
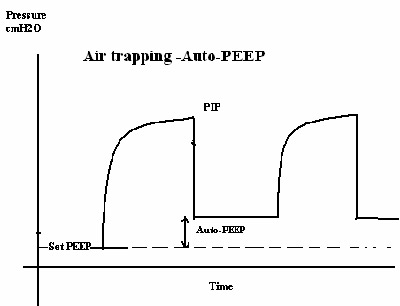
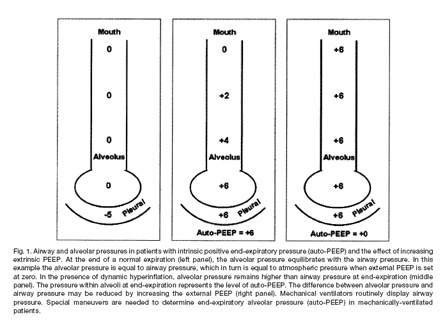
Air Trapping (auto-PEEP)
Causes:
- increased exp resistance (either in the airways or in the circuit)-thick secretion , bronchospasm
- Insufficient expiratory time
- Early collapse of unstable alveoli/airways during exhalation
How to identify it on the graphics
- Pressure time: while performing an expiratory hold, the waveform rises above baseline
- Flow-time: the exp flow doesn't return to baseline before the next breath begins
- Volume-time: the exp portion doesn't return to baseline
- FV Loop: the loop doesn't meet at the baseline
- PV Loop: the loop doesn't meet at the baseline
How to Fix:
- ID the cause and resolve
- Give a treatment, suction, decrease It/increase flow, add PEEP
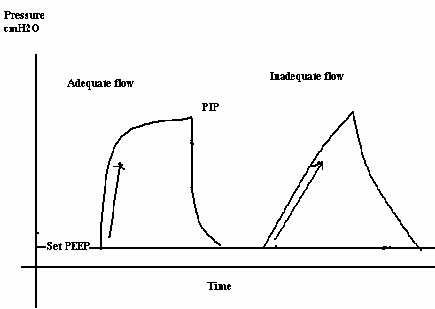
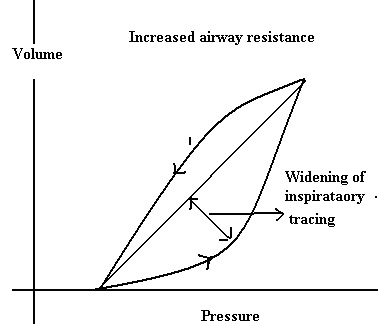
Airway Resistance Changes
Causes:
- Bronchospasm
- Damp or blocked expiratory valve/filter
- ETT problems (too small, kinked, obstructed, patient biting)
- High flow
- Secretion build-up
- Water in the HME
How to identify
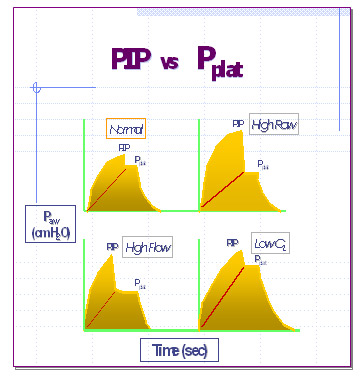
- Pressure-time: the PIP increases but the plateau stays the same
- Volume-time: it takes longer for the exp curve to reach the baseline
- Flow-time: it takes longer for the exp curve to reach baseline and the exp flow rate is reduced
- FV loop: decreased exp flow with a scoop in the exp curve
- PV loop: the loop will be fatter.if it bulges to the right, it's insp resistance and to the left it's exp
How to fix
- ID cause and fix it
- Give a tx, sx, drain water, change HME, change ETT, add a bite block, decrease PF rate, change exp filter
Compliance changes
Causes
- ARDS
- Atelectasis
- Abdominal distension
- CHF
- Consolidation
- Fibrosis
- Hyperinflation
- Pneumothorax
- Pleural effusion
- Just about every pulm dx there is
How to identify it
- Pressure-time: the PIP and plateau both increase
- PV loop: lays more horizontal
- Increased compliance
Causes
- Surfactant therapy, natural resolution pneumonia , ICD draining of pneumothorax
How to identify it
- Pressure-time: PIP and plateau both decrease
- PV loop: stands more vertical (upright)
Active Exhalation
- Causes
Patient is exhaling below FRC due to air trapping (vol dumping)
Pain
Positional change
Equipement calibration problem
- How to identify it
Volume-time: exp waveform goes below the baseline
PV loop: exp loop goes past the zero point
FV loop: exp part goes past the zero point
- How to fix it
Reduce air-trapping
Calibrate equipment
Relieve pain
Partial Obstruction
- Causes
Suction catheter left in ETT
Tissue flap
Mucus plug
Water/secretions in the circuit or airway
- How to identify It
Flow-volume: flow is not steady and constant, but varies as the obst moves around
PV loop: jagged instead of smooth
FV loop: jagged with fluctuating flow
- How to fix it
Pull catheter out of ETT
Suction
Drain water
Change HME
Move the ETT
Overdistension
- Causes
Vt set too high (vol vent)
Pressure set too high (press vent)
Could occur in pressure vent with C or Raw changes
- How to identify it
PV loop: bird beak at the top of the loop
- How to fix it
Reduce Vt (vol vent)
Reduce pressure (P vent)
Leak
- Causes
Expiratory leak: air leak through a chest tube, BP fistula, ETT cuff leak, NG tube in trachea
Inspiratory leak: loose connections, ventilator malfunction, faulty flow sensor
- How to identify it
Pressure-time: decreased PIP
Volume-time: decreased Vt.exp leaks keep exp Vt from returning to baseline
Flow-time: PEF decreases
PV loop: exp side doesn't return to the baseline
FV loop: exp part doesn't return to baseline
- How to fix it
Identify source of leak and fix it
Do a leak test and make sure all connections are tight
Back







